mannitol injection, USP
Find mannitol injection, USP medical information:
Find mannitol injection, USP medical information:
mannitol injection, USP Quick Finder
Highlights
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use MANNITOL INJECTION safely and effectively. See full prescribing information for MANNITOL INJECTION. MANNITOL injection, for intravenous use Initial U.S. Approval: 1964 RECENT MAJOR CHANGESINDICATIONS AND USAGEDOSAGE AND ADMINISTRATIONAdministration Instructions (2.1):
Recommended Dosage (2.2):
DOSAGE FORMS AND STRENGTHSMannitol Injection 25%, USP: 12.5 g/50 mL (0.25 g/mL) in a single-dose vial (3) CONTRAINDICATIONSWARNINGS AND PRECAUTIONS
ADVERSE REACTIONSMost common adverse reactions are hypersensitivity reactions, renal failure, CNS toxicity, hypo/hypervolemia, hypo/hypernatremia, hypo/hyperkalemia, and infusion site reactions. (6) To report SUSPECTED ADVERSE REACTIONS, contact Hospira, Inc. at 1-800-441-4100 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch. DRUG INTERACTIONS
See 17 for PATIENT COUNSELING INFORMATION. Revised: 3/2020 |
Indications and Usage
Dosage and Administration
2 DOSAGE AND ADMINISTRATION
2.1 Important Preparation and Administration Instructions
- Mannitol Injection is for intravenous infusion preferably through a central venous catheter [see Warnings and Precautions (5.6), Description (11)].
- Prior to the administration of Mannitol Injection, evaluate renal, cardiac, and pulmonary status of the patient and correct fluid and electrolyte imbalances [see Dosage and Administration (2.2)].
- Do not administer Mannitol Injection simultaneously with blood products or through the same administration set because of the possibility of pseduoagglutination or hemolysis. If it is essential that blood be given simultaneously, at least 20 mEq of sodium chloride should be added to each liter of mannitol solution to avoid pseudoagglutination.
- Do not transfer Mannitol Injection into polyvinylchloride (PVC) bags; a white flocculent precipitate may form from contact with PVC surfaces.
- Administer Mannitol Injection using an administration set with a filter to ensure against infusion of mannitol crystals.
Preparation
- Visually inspect the container before preparation and again before administration. Do not administer unless solution is clear, the container undamaged, and the fliptop vial seal intact.
- Crystals may form in Mannitol Injection, especially if the solution is exposed to low temperatures. If crystallization occurs, warm the vial in water at 80°C and periodically shake vigorously to dissolve the crystals. Mannitol Injection may be autoclaved at 121°C for 20 minutes at 15 psi. Cool to body temperature or less before administering. Re-inspect Mannitol Injection for crystals prior to administration. Discard the solution if all the crystals cannot be dissolved.
- Remove cover from fliptop vial and cleanse stopper with antiseptic before use.
- Additives may be incompatible. Consult with pharmacist, if available.
- For single use only; discard unused portion.
2.2 Recommended Dosage
Prior to administration of Mannitol Injection, evaluate renal, cardiac, and pulmonary status of the patient and correct fluid and electrolyte imbalances.
The total dosage, concentration, and rate of administration depend on the age, weight, and condition of the patient being treated, including fluid requirement, electrolyte balance, serum osmolality, urinary output, and concomitant therapy.
The following outline of administration and dosage is only a general guide to therapy.
Reduction of Intracranial Pressure and Treatment of Cerebral Edema
Usually a maximum reduction in intracranial pressure can be achieved with a dose of 0.25 g/kg administered as an intravenous infusion over at least 30 minutes, which may be repeated every six to eight hours. During and following infusion of Mannitol Injection, monitor fluid and electrolytes, serum osmolarity, and renal, cardiac, and pulmonary function. Discontinue Mannitol Injection if renal, cardiac, or pulmonary status worsens or CNS toxicity develops [see Warnings and Precautions (5.2, 5.3, 5.4, 5.5)].
Reduction of Intraocular Pressure
The recommended dosage is 1.5 to 2 g/kg as a single dose administered as an intravenous infusion over at least 30 minutes. When used preoperatively, administer Mannitol Injection 60 to 90 minutes before surgery to achieve maximal reduction of intraocular pressure before operation.
Dosage Forms and Strengths
Contraindications
4 CONTRAINDICATIONS
Mannitol Injection is contraindicated in patients with:
- Known hypersensitivity to mannitol [see Warnings and Precautions (5.1)].
- Anuria [see Warnings and Precautions (5.2)].
- Severe hypovolemia [see Warnings and Precautions (5.4)].
- Pre-existing severe pulmonary vascular congestion or pulmonary edema [see Warnings and Precautions (5.5)].
- Active intracranial bleeding except during craniotomy.
Warnings and Precautions
5 WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity Reactions
Serious hypersensitivity reactions, including anaphylaxis, hypotension, and dyspnea resulting in cardiac arrest and death have been reported with Mannitol Injection [see Adverse Reactions (6)]. Stop the infusion immediately if signs or symptoms of a suspected hypersensitivity reaction develop. Initiate appropriate therapeutic countermeasures as clinically indicated.
5.2 Renal Complications Including Renal Failure
Renal complications, including irreversible renal failure, have been reported in patients receiving mannitol.
Reversible, oliguric acute kidney injury has occurred in patients with normal pretreatment renal function who received large intravenous doses of mannitol. Although the osmotic nephrosis associated with mannitol administration is in principle reversible, osmotic nephrosis in general is known to potentially proceed chronic or even end-stage renal failure. Monitor renal function closely, including signs of urine output reduction, during mannitol injection.
Patients with pre-existing renal disease, patients with conditions that put them at risk for renal failure, or those receiving potentially nephrotoxic drugs or other diuretics, are at increased risk for renal failure following administration of Mannitol Injection. Avoid concomitant administration of nephrotoxic drugs (e.g., aminoglycosides) or other diuretics with Mannitol Injection, if possible [see Drug Interactions (7)].
Patients with oliguric acute kidney injury who subsequently develop anuria while receiving mannitol are at risk of congestive heart failure, pulmonary edema, hypertensive crisis, coma, and death.
During and following infusion of Mannitol Injection for the reduction in intracranial pressure, monitor the patient clinically and laboratory tests for changes in fluid and electrolyte status. Discontinue Mannitol Injection if renal function worsens [see Warnings and Precautions (5.5)].
5.3 Central Nervous System (CNS) Toxicity
CNS toxicity manifested by, e.g., confusion, lethargy, coma, has been reported in patients treated with mannitol, some resulting in death, in particular in the presence of impaired renal function CNS toxicity may result from high serum mannitol concentrations, serum hyperosmolarity resulting in intracellular dehydration within CNS, hyponatremia or other disturbances of electrolyte and acid/base balance secondary to mannitol administration [see Warnings and Precautions (5.4)].
At high concentrations, mannitol may cross the blood brain barrier and interfere with the ability of the brain to maintain the pH of the cerebrospinal fluid especially in the presence of acidosis.
In patients with pre-existing compromise of the blood brain barrier, the risk of increasing cerebral edema (general and focal) associated with repeated or continued use of Mannitol Injection must be individually weighed against the expected benefits.
A rebound increase of intracranial pressure may occur several hours after the infusion. Patients with a compromised blood brain barrier are at increased risk.
Concomitant administration of neurotoxic drugs (e.g., aminoglycosides) with Mannitol Injection may potentiate neurotoxicity. Avoid concomitant use of neurotoxic drugs, if possible [see Drug Interactions (7.3)].
During and following infusion of Mannitol Injection for the reduction in intracranial pressure, monitor the patient clinically and laboratory tests for changes in fluid and electrolyte status. Discontinue Mannitol Injection if CNS toxicity develops [see Warnings and Precautions (5.5)].
5.4 Fluid and Electrolyte Imbalances, Hyperosmolarity
Depending on dosage and duration, administration of Mannitol Injection may result in hypervolemia leading to or exacerbating existing congestive heart failure. Accumulation of mannitol due to insufficient renal excretion increases the risk of hypervolemia. Mannitol-induced osmotic diuresis may cause or worsen dehydration/hypovolemia and hemoconcentration. Administration of Mannitol Injection may also cause hyperosmolarity [see Description (11)].
Depending on dosage and duration of administration, electrolyte and acid/base imbalances may also result from transcellular shifts in water and electrolytes, osmotic diuresis, and/or other mechanisms. Such imbalances may be severe and potentially fatal.
Imbalances that may result from administration of Mannitol Injection include:
- Hypernatremia, dehydration, and hemoconcentration
- Hyponatremia, which can lead to headache, nausea, seizures, lethargy, coma, cerebral edema, and death. Acute symptomatic hyponatremic encephalopathy is considered a medical emergency.
- Hypo/hyperkalemia. The development of electrolyte imbalances (e.g., hyperkalemia, hypokalemia) associated with mannitol administration may result in cardiac adverse reactions in patients receiving drugs that are sensitive to such imbalances (e.g., digoxin, agents that may cause QT prolongation, neuromuscular blocking agents) [see Drug Interactions (7.4)].
- Other electrolyte disturbances
- Metabolic acidosis/alkalosis
Pediatric patients less than two years of age, particularly preterm and term neonates, may be at higher risk for fluid and electrolyte abnormalities following administration of Mannitol Injection due to decreased glomerular filtration rate and limited ability to concentrate urine [see Use in Specific Populations (8.4)].
During and following infusion of Mannitol Injection for the reduction in intracranial pressure, monitor fluid and electrolyte status and discontinue Mannitol Injection if imbalances occur [see Warnings and Precautions (5.5)].
5.5 Monitoring/Laboratory Tests
During and following infusion of Mannitol Injection for the reduction in intracranial pressure, monitor:
- serum osmolarity, serum electrolytes (including sodium, potassium, calcium and phosphate) and acid/base balance,
- the osmol gap
- signs of hypo- or hypervolemia, including urine output
- renal, cardiac, and pulmonary function
- intracranial pressure
Discontinue Mannitol Injection if renal, cardiac, or pulmonary status worsens or CNS toxicity develops [see Contraindications (4)].
5.6 Infusion Site Reactions
The infusion of hypertonic solutions through a peripheral vein, including Mannitol Injection, may result in peripheral venous irritation, including phlebitis. Other severe infusion site reactions, such as compartment syndrome and swelling associated with extravasation, can occur with administration of Mannitol Injection [see Adverse Reactions (6)]. Mannitol Injection is preferably administered through a central venous catheter [see Dosage and Administration (2.1)].
5.7 Interference with Laboratory Tests
High concentrations of mannitol can cause false low results for inorganic phosphorus blood concentrations [see Drug Interactions (7.6)].
Mannitol may produce false positive results in tests for blood ethylene glycol concentrations [see Drug Interactions (7.6)].
Adverse Reactions
6 ADVERSE REACTIONS
The following adverse reactions associated with the use mannitol were identified in clinical studies or postmarketing reports. Because some of these reactions were reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
| Hypersensitivity reactions: | Cardiac arrest, anaphylaxis, hypotension, dyspnea, hypertension, pyrexia, chills, sweating, cough, musculoskeletal stiffness, myalgia, urticaria/rash, pruritus, generalized pain, discomfort, nausea, vomiting, headache [see Warnings and Precautions (5.1)] |
| Renal failure: | Acute kidney injury, osmotic nephrosis, anuria, oliguria, urinary retention [see Warnings and Precautions (5.2)] |
| CNS toxicity: | Coma, seizures, confusion, lethargy, rebound increase in intracranial pressure, headache, dizziness [see Warnings and Precautions (5.3)] |
| Fluid and electrolyte imbalances: | Metabolic acidosis, dehydration (hypovolemia), hypervolemia, hyponatremia, hypernatremia, hyperkalemia, hypokalemia [see Warnings and Precautions (5.4)] |
| Infusion site reactions: | Venous thrombosis, thrombophlebitis extending from the site of injection, compartment syndrome and swelling associated with extravasation [see Warnings and Precautions 5.6)] |
| Cardiac and respiratory disorders: | Tachycardia, angina-like chest pain, congestive heart failure, pulmonary congestion, hypotension, edema, rhinitis |
| Gastrointestinal disorders: | Dryness of mouth, nausea, vomiting |
| General disorders: | Thirst |
Drug Interactions
7 DRUG INTERACTIONS
7.1 Nephrotoxic Drugs
Concomitant administration of nephrotoxic drugs (e.g., cyclosporine, aminoglycosides) increases the risk of renal failure following administration of mannitol. Avoid use of nephrotoxic drugs with Mannitol Injection, if possible [see Warnings and Precautions (5.2)].
7.2 Diuretics
Concomitant administration of other diuretics may potentiate the renal toxicity of mannitol. Avoid concomitant administration of other diuretics with Mannitol Injection, if possible [see Warnings and Precautions (5.2)].
7.3 Neurotoxic Drugs
Concomitant administration of systemic neurotoxic drugs (e.g., aminoglycosides) with Mannitol Injection may potentiate the CNS toxicity of mannitol. Avoid use of systemic neurotoxic drugs with Mannitol Injection, if possible [see Warnings and Precautions (5.3)].
7.4 Drugs Affected by Electrolyte Imbalances
The development of electrolyte imbalances (e.g., hyperkalemia, hypokalemia) associated with mannitol administration may result in cardiac adverse reactions in patients receiving drugs that are sensitive to such imbalances (e.g., digoxin, drugs that prolong the QT interval, neuromuscular blocking agents) [see Warnings and Precautions (5.4)]. During and following infusion of Mannitol Injection, monitor serum electrolytes and discontinue Mannitol Injection if cardiac status worsens [see Warnings and Precautions (5.5)].
7.5 Renally Eliminated Drugs
Mannitol therapy may increase the elimination, and decrease the effectiveness of treatment with, drugs that undergo significant renal elimination. Concomitant administration of mannitol with lithium may initially increase the elimination of lithium but may also increase the risk of lithium toxicity if patients develop hypovolemia or renal impairment. In patients receiving lithium, consider holding lithium doses during treatment with Mannitol Injection. In patients requiring concomitant administration of lithium and Mannitol Injection, frequently monitor serum lithium concentrations and for signs of lithium toxicity.
7.6 Interference with Laboratory Tests
High concentrations of mannitol can cause false low results for inorganic phosphorus blood concentrations when an assay based on the conversion of phosphate (orthophosphate) to the phosphomolybdate complex is used.
Mannitol may produce false positive results in tests for blood ethylene glycol concentrations in which mannitol is initially oxidized to an aldehyde.
Use in Specific Populations
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
The available case report data with mannitol over decades of use have not identified a drug-associated risk of major birth defects, miscarriage or adverse maternal or fetal outcomes. Mannitol crosses the placenta and may cause fluid shifts that could potentially result in adverse effects in the fetus (see Data).No adverse developmental effects from mannitol were reported in published animal studies; however, fluid shifts occurred in fetal ewes in response to maternal infusion of mannitol.
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2 to 4% and 15 to 20%, respectively.
8.2 Lactation
Risk Summary
There are no data on the presence of mannitol in either human or animal milk, the effects on the breastfed infant, or the effects on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for Mannitol Injection and any potential adverse effects on the breastfed child from Mannitol Injection or from the underlying maternal condition.
8.4 Pediatric Use
Mannitol Injection is approved for use in the pediatric population for the reduction of intracranial and intraocular pressure. Studies have not defined the optimal dose of Mannitol Injection in the pediatric population. The safety profile for mannitol use in pediatric patients is similar to adults at dosages described in labeling. However, pediatric patients less than two years of age, particularly preterm and term neonates, may be at higher risk for fluid and electrolyte abnormalities following administration of Mannitol Injection due to decreased glomerular filtration rate and limited ability to concentrate urine [see Warnings and Precautions (5.4)].
8.5 Geriatric Use
Mannitol is known to be substantially excreted by the kidney, and the risk of adverse reactions to this drug may be greater in elderly patients with impaired renal function. Evaluate the renal, cardiac and pulmonary status of the patient and correct fluid and electrolyte imbalances prior to administration of Mannitol Injection [see Warnings and Precautions (5.2, 5.3, 5.4, 5.5)].
8.6 Renal Impairment
Patients with pre-existing renal disease, patients with conditions that put them at high risk for renal failure, or those receiving potentially nephrotoxic drugs or other diuretics, are at increased risk of renal failure with administration of mannitol. Evaluate the renal, cardiac, and pulmonary status of the patient and correct fluid and electrolyte imbalances prior to administration of Mannitol Injection [see Warnings and Precautions (5.2, 5.3, 5.4, 5.5)].
Overdosage
10 OVERDOSAGE
Signs and symptoms of overdose with Mannitol Injection include renal failure and acute kidney injury, hypo/hypervolemia, hyperosmolarity and electrolyte imbalances, CNS toxicity (e.g., coma, seizures), some of which can be fatal [see Warnings and Precautions (5.2, 5.3, 5.4)].
Management of overdosage with Mannitol Injection is symptomatic and supportive. Discontinue the infusion and institute appropriate corrective measures with particular attention to renal, cardiac, and pulmonary systems. Correct fluid and electrolyte imbalances.
Mannitol Injection is dialyzable (hemodialysis and peritoneal dialysis), hemodialysis may increase mannitol elimination.
Description
11 DESCRIPTION
Mannitol Injection, USP is a sterile, nonpyrogenic solution of mannitol in water for injection available in a fliptop vial for intravenous administration as an osmotic diuretic.
The content and characteristics are as follows:
| Conc. (%) | g/100 mL | mOsmol/liter (calc.) | pH* |
|---|---|---|---|
| |||
| 25 | 25 | 1372 | 5.9 (4.5 to 7.0) |
The solution contains no bacteriostat, antimicrobial agent, or added buffer (except for pH adjustment) and is intended only as a single-dose injection.
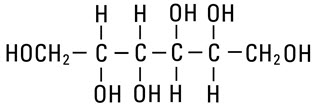
Mannitol, USP is chemically designated D-mannitol (C6H14O6), a white crystalline powder or free-flowing granules freely soluble in water. It has the following structural formula:
Water for Injection, USP is chemically designated H2O.
Clinical Pharmacology
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Mannitol, when administered intravenously, exerts its osmotic diuretic effect as a solute of relatively small molecular size largely confined to the extracellular space. Mannitol hinders tubular reabsorption of water and enhances excretion of sodium and chloride by elevating the osmolarity of the glomerular filtrate.
This increase in extracellular osmolarity affected by the intravenous administration of mannitol will induce the movement of intracellular water to the extracellular and vascular spaces. This action underlies the role of mannitol in reducing intracranial pressure, intracranial edema, and intraocular pressure.
12.3 Pharmacokinetics
Distribution
Mannitol distributes largely to the extracellular space within 20 to 40 minutes after intravenous administration. The volume of distribution of mannitol is approximately 17 L in adults.
Elimination
In subjects with normal renal function, the total clearance is 87 to 109 mL/minute. The elimination half-life of mannitol is 0.5 to 2.5 hours
Metabolism
Only a relatively small amount of the mannitol dose is metabolized after intravenous administration to healthy subjects.
Excretion
Mannitol is eliminated primarily via the kidneys in unchanged form. Mannitol is filtered by the glomeruli, exhibits less than 10% of tubular reabsorption, and is not secreted by tubular cells. Following intravenous administration, approximately 80% of an administered dose of mannitol is estimated to be excreted in the urine in 3 hours with lesser amounts thereafter.
Specific Populations
Patients with Renal Impairment
In patients with renal impairment, the elimination half-life of mannitol is prolonged. In a published study, in patients with renal impairment including acute renal failure and end stage renal failure, the elimination half-life of mannitol was estimated at about 36 hours, based on serum osmolarity. In patients with renal impairment on dialysis, the elimination half-life of mannitol was reduced to 6 and 21 hours during hemodialysis and peritoneal dialysis, respectively [see Use in Specific Populations (8.6), Overdosage (10)].
How Supplied/Storage and Handling
Patient Counseling Information
17 PATIENT COUNSELING INFORMATION
Inform patients or caregivers of the following risks of Mannitol Injection:
- Hypersensitivity Reactions [see Warnings and Precautions (5.1)]
- Renal Complications Including Renal Failure [see Warnings and Precautions (5.2)].
- CNS Toxicity [see Warnings and Precautions (5.3)]
- Fluid and Electrolyte Imbalances, Hyperosmolarity [see Warnings and Precautions (5.4)]
- Infusion Site Reactions [see Warnings and Precautions (5.6)]
Other

17 PATIENT COUNSELING INFORMATION
17 PATIENT COUNSELING INFORMATION
Inform patients or caregivers of the following risks of Mannitol Injection:
- Hypersensitivity Reactions [see Warnings and Precautions (5.1)]
- Renal Complications Including Renal Failure [see Warnings and Precautions (5.2)].
- CNS Toxicity [see Warnings and Precautions (5.3)]
- Fluid and Electrolyte Imbalances, Hyperosmolarity [see Warnings and Precautions (5.4)]
- Infusion Site Reactions [see Warnings and Precautions (5.6)]
Resources
Didn’t find what you were looking for?
Contact us.
Chat online with Pfizer Medical Information regarding your inquiry on a Pfizer medicine.
*Speak with a Pfizer Medical Information Professional regarding your medical inquiry. Available 9AM-5PM ET Monday to Friday; excluding holidays.
Submit a medical question for Pfizer prescription products.
Report Adverse Event
Pfizer Safety
To report an adverse event related to a Pfizer product and you are not part of a clinical trial* for this product, click the link below to submit your information: Pfizer Safety Reporting Site
*If you are involved in a clinical trial for either product, adverse events should be reported to your coordinating study site.
If you cannot use the above website to report an adverse event related to a Pfizer product, please call Pfizer Medical Information at (800) 438-1985.
FDA Medwatch
You may also contact the U.S. Food and Drug Administration (FDA) directly to report adverse events or product quality concerns either online at www.fda.gov/medwatch or by calling (800)-332-1088.